
On December 14th Health Secretary Matt Hancock announced in parliament that a new variant of COVID-19 had been identified and was spreading much faster in some areas across the country. There was statistical evidence of an increasing surge in the transmission rate in Kent, which is where a new COVID-19 strain ‘B.1.1.7’ was detected.
The B.1.1.7 COVID-19 mutation is reported to have many changes from the original form of COVID-19. There is a hypothesis that this mutation originated in a chronically infected patient, but no clarity on the geographical source. While the first discovery was made in the county of Kent in the UK, this may not be the origin. It is likely that this, or other variants are already spreading world-wide. The World Health Authority was notified immediately the discovered mutation was confirmed in the UK. There have also been reports of a different mutation being discovered in South Africa.

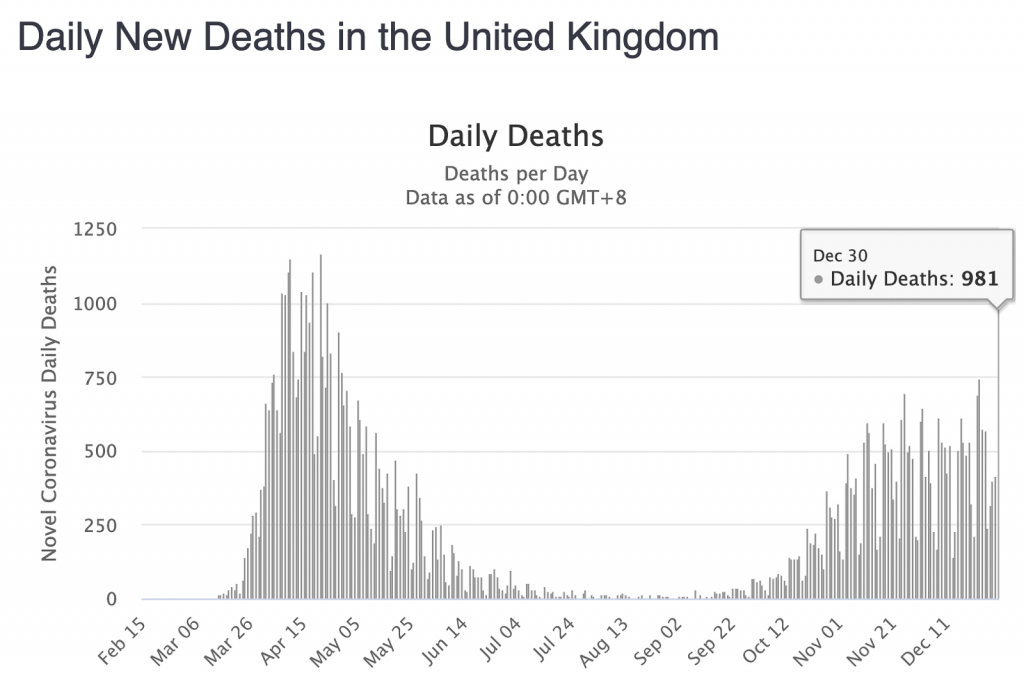
Graph of Spread>
It was on 18th December that the ‘New and Emerging Respiratory Virus Threats Advisory Group’ provided the government with the formal evidence that the COVID-19 mutation had a 70% higher transmission rate. The next day, on 19th December, Boris Johnson announced a new ‘Tier 4’ lockdown to the country and confirmed that Christmas celebrations would need to take place within family bubbles, i.e. no mixing between households.
As we approached Christmas, the accelerated spread of the new strain was alarming and the rapid increase in the number of daily deaths in the UK makes for grim reading.
The graphs need no explanation.
Writing this post at the end of the month, I understand that the NHS is now beyond peak capacity in some areas. Critical care capacity in London and South East was reported at 110% and a couple of days ago and a ‘major incident’ was declared in Essex.
Ambulances are queuing for hours at some hospitals with staff providing treatment to incoming patients inside the waiting ambulances. Patients in Kent are being redirected to Surrey and beyond. Patients in London are being taken as far away as Yorkshire. I heard on the radio yesterday that the NHS still has over 100,000 unfilled posts. This can only get worse in the short-term as we leave the European Union and all of those European workers head back home.
NHS staff sickness due to COVID infection (and having to self-isolate) is a massive problem. Absences are between 8% and 12% across regions. Frontline staff are having to work extra hours, under intense pressure and seeing their annual leave requests being cancelled.
News about the Nightingale hospitals is non-existent this month. Perhaps there aren’t enough front-line NHS staff available to make them operational?
With two vaccines now coming on stream, there is some light at the end of the tunnel. How-ever there are major challenges to be overcome before we can get any-where near the desired level of ‘herd immunity’. The suppliers a gearing up production and putting distribution channels in place to deliver vaccines across the entire world.
In the UK we are dealing with the challenges of establishing necessary logistics across the country, and creating the communications and management for our population of 66.65M (ranked in priority order) and putting in place a very large team of suitably skilled/experienced people to administer both doses of the vaccine
It is now a race against time and the accelerating spread of the mutated virus. The immediate future is looking precarious, the statistics are already grim.

COVID-19 Global Cases dashboard, built and maintained by John Hopkins University Centre for Science and Engineering. Click through for the latest updates / live position.
References and other useful links are as follows:
Technical description of B.1.1.7 detected in the UK with additional references on this link.
NHS COVID-19 advice can be found on: https://www.nhs.uk/conditions/coronavirus-covid-19/
Worldometer Coronavirus update: https://www.worldometers.info/coronavirus/
DataBrew home page: https://www.datacat.cc/covid/





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}